Cancer interception refers to the idea of interrupting carcinogenesis at any point before the development of an invasive disease. Nowadays, most people think that cancer prevention is a passive process that requires avoiding risk factors (e.g. tobacco smoke) to prevent the development of the disease (e.g. lung cancer). This is called “primary prevention”, and is fundamental. However, in recent years the importance of other approaches has antihypertensive agents in high-risk patients with severe hypertension or with class III/IV heart failure, the use of statins in patients with prior myocardial infarction and very high low-density lipoprotein (LDL) cholesterol, and the use of aspirin in patients with prior MI or stroke are the first success stories in the field. Once effective therapies in advanced disease, now all these strategies are CVD prevention standards.
Instead, up to now the idea of cancer interception has been a hard sell, even among educated people prone to trying active prevention for their personal health. Troubles with adherence to risk reduction-based approaches (e.g. the use of effective breast cancer risk-reducing agents) are around the corner. One proposed hindrance is the risk of toxic effects, such as adverse cardiovascular effects produced by nonsteroidal anti-inflammatory drugs (NSAIDs, for example celecoxib) when utilized to intercept colorectal neoplasia.
However, low-baseline CVD risk or C-reactive protein level (a well established marker of inflammation) eliminate this risk, highlighting, at the same time, the importance of a more personalized cancer interception. Interestingly, the use of antihypertensive drugs to reduce CVD is associated with toxicity risk too. The general acceptance of this risk highlights the need to fill the gap between the education on CVD risk reduction and the education on cancer risk reduction.
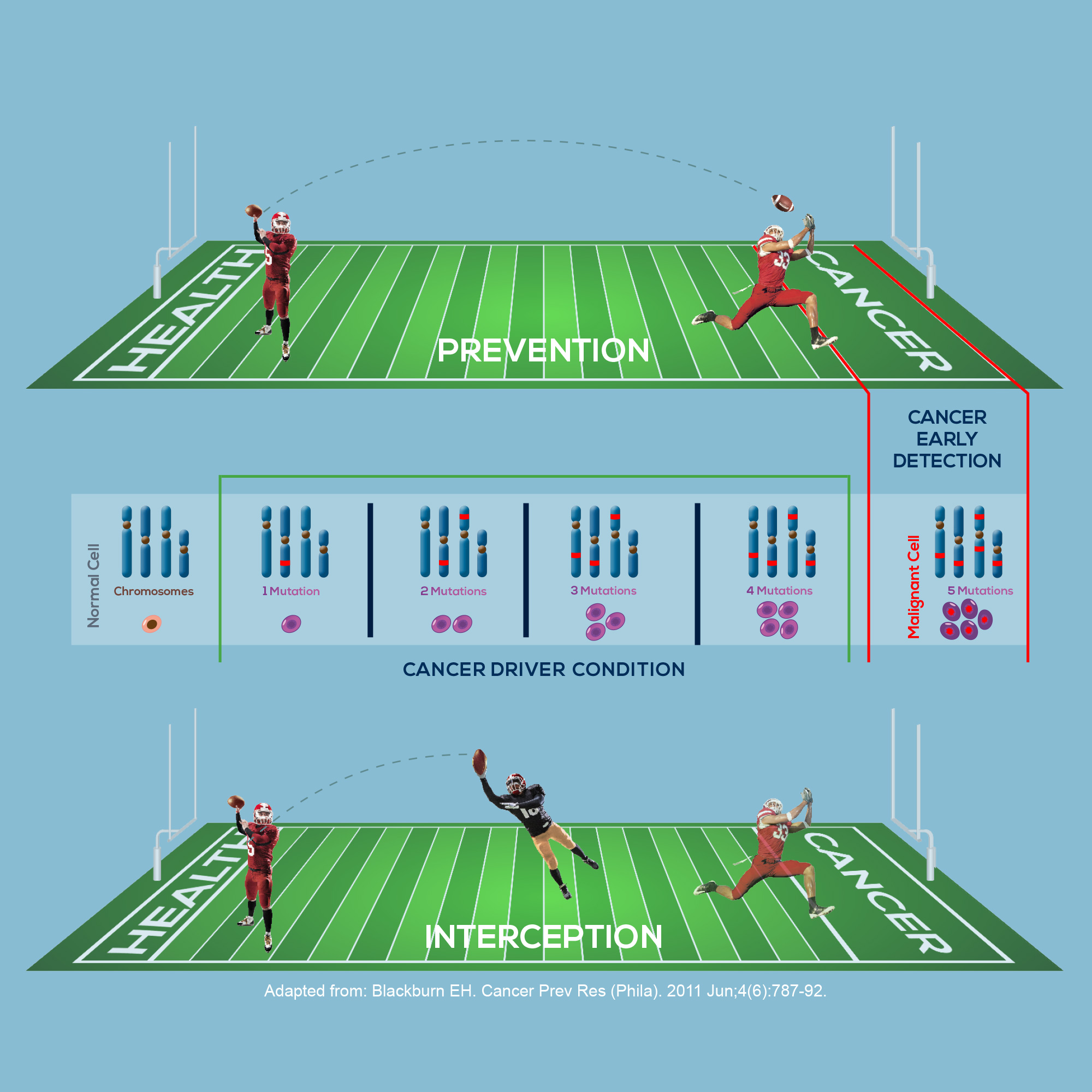
Another proposed reason behind the resistance to the idea of cancer interception is that whereas CVD risk reduction treats well-known measurable conditions (such as hypertension and high cholesterol level) that can be followed to assess treatment effectiveness, actionable cancer drivers and prodromal conditions are less known by the general population. Actually, there is at least one good example of an actionable measurable condition for cancer too: colorectal adenomas preceding colon cancer. Their number can be reduced by aspirin, which has been shown to reduce the incidence and the mortality from colorectal cancer. Also, surgical control of colorectal adenomas can reduce cancer risk and mortality.
Understandably, people struggle with treating or even curing cancer. However, cancer will never be controlled without prevention. This is why cancer interception is absolutely desirable and necessary.